Introduction
When someone experiences a stroke, 1.9 million neurons die every minute without treatment. During this critical window, how a patient is transported can determine whether they regain function or face permanent disability.
"Transporting a stroke patient" isn't one situation — it's several. You might be calling 911 during an acute episode, physically moving a patient to a vehicle, arranging a transfer between facilities, or scheduling ongoing rides to rehab. Each scenario calls for a different response.
This guide covers:
- When to call 911 vs. arrange non-emergency transport
- Step-by-step process for moving a stroke patient safely
- Physical handling techniques to prevent injury
- Common mistakes families and caregivers make
- How to choose the right transport method for your situation
TLDR
- Always call 911 for suspected acute stroke — never drive the patient yourself
- Time windows for treatment (tPA within 3–4.5 hours, thrombectomy up to 24 hours) make speed critical
- Transfer toward the unaffected side and never pull on the weakened arm
- For post-hospital needs, non-emergency medical transport (NEMT) is safer than personal vehicles
- Having the patient's medications, medical records, and care instructions ready before transport reduces delays and prevents avoidable complications
How to Transport a Stroke Patient: Step-by-Step
Step 1: Recognize Stroke Symptoms and Activate Emergency Services
Use the FAST acronym to identify stroke quickly:
- Face drooping on one side
- Arm weakness or inability to raise both arms
- Speech difficulty, slurred words, or confusion
- Time to call 911 immediately
Other warning signs include sudden severe headache, vision changes, or loss of balance.
Call 911 immediately — do not attempt to drive the patient to the hospital yourself. EMS can begin assessment during transport and notify the receiving stroke center before arrival, saving critical treatment time.
Note the exact time symptoms first appeared. This timestamp determines eligibility for clot-busting medication (tPA) and other interventions. If you don't know when symptoms began, note the last time the patient was "normal."
Step 2: Keep the Patient Safe and Calm While Waiting for EMS
Do not give the patient food, water, or medication while waiting. Stroke patients often develop swallowing difficulties that create aspiration risk — even a sip of water can be dangerous before medical assessment.
If the patient is conscious, help them lie down or sit in a supported, comfortable position. Keep them calm, reassured, and still to avoid unnecessary exertion or agitation.
If the patient is unconscious and breathing, place them in the recovery position (on their side). If not breathing, begin CPR if trained to do so.
Step 3: Brief EMS on the Patient's Condition
When EMS arrives, provide three critical pieces of information:
- Time of symptom onset — the exact time you first noticed symptoms or when the patient was last normal
- Medical history — current medications (especially blood thinners), prior strokes, diabetes, heart conditions
- Current observations — weakness on one side, slurred speech, confusion, level of consciousness
This information helps EMS assess the situation and select the right destination — not all hospitals can perform advanced stroke interventions.
Stroke center type makes a real difference in treatment options. EMS triage protocols directly influence which facility the patient is taken to, and getting to the right center the first time can determine whether certain treatments are even available:
- Primary Stroke Center (PSC) — administers tPA and provides standard stroke care
- Thrombectomy-Capable Stroke Center (TSC) — performs mechanical clot removal up to 24 hours after onset
- Comprehensive Stroke Center (CSC) — handles the most complex cases with full interventional capabilities
Step 4: Use Safe Physical Handling and Transfer Techniques
Every transfer — bed to stretcher, chair to vehicle — carries real injury risk for stroke patients. Follow these handling rules:
- Transfer toward the stronger side — always move the patient in the direction of their unaffected limb for better stability
- Never pull the weakened arm — use a transfer belt at the waist instead, and angle the destination surface at 45 degrees for a pivot transfer
- Use two people or a mechanical lift when the patient has poor trunk control, balance problems, or unpredictable movement post-stroke
- Don't attempt a solo transfer if there's any uncertainty about safety

Support the affected arm throughout the transfer. Hemiplegic shoulder pain affects up to 47% of stroke patients, and it's often caused when a flaccid arm is allowed to dangle or be pulled during transfers.
Step 5: Monitor the Patient Continuously During Transport
Keep the patient positioned with the head and torso slightly elevated (30 degrees) unless otherwise directed by medical staff. This helps manage blood pressure and reduces aspiration risk.
During transport, watch for:
- Changes in consciousness or responsiveness
- Breathing difficulty or seizure activity
- Any sudden worsening of stroke symptoms
Report anything new immediately to EMS or the accompanying medical personnel. Beyond monitoring, keep the environment calm and the ride as smooth as possible — sudden stops or aggressive movement can cause anxiety, pain, or injury in a neurologically compromised patient.
Key Safety Considerations When Transporting a Stroke Patient
Stroke patients present unique challenges during transport:
- One-sided weakness (hemiplegia)
- Impaired sensation
- Visual field deficits
- Communication difficulties (aphasia)
- Unpredictable cognitive changes
Knowing these conditions upfront shapes every decision — from how you position the patient to how you speak to them en route.
Positioning and Comfort
Safe positioning reduces the risk of secondary complications during transport:
- Keep the head elevated at approximately 30 degrees to regulate intracranial pressure and reduce aspiration risk — avoid flat positioning unless medically directed
- Support the affected or flaccid arm on a surface, sling, or lap tray to prevent shoulder subluxation and pain
- Ensure seatbelts and straps are secure but not pressing on the weakened side
Physical positioning is only part of the picture. How you communicate with a stroke patient matters just as much.
Communication with the Patient
Stroke patients with aphasia can understand more than they can express. Always speak calmly, use simple sentences, and offer visual cues or gestures to reduce anxiety and help the patient feel at ease during the trip.
Never assume an unresponsive or confused patient cannot hear or understand — maintain respectful, clear communication from pickup to drop-off.
Common Mistakes When Transporting a Stroke Patient
Even well-intentioned decisions can slow treatment or cause harm. Here are the most common errors to avoid:
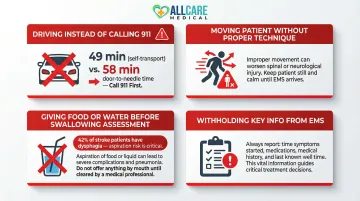
- Driving to the hospital instead of calling 911: EMS can begin assessment en route and pre-notify the stroke center — two steps a private vehicle can't replicate. Patients transported by EMS receive tPA faster than those arriving by private vehicle, with median door-to-needle times of 49 versus 58 minutes.
- Moving the patient too quickly or without proper technique: Pulling on the affected arm, skipping a transfer belt, or attempting a solo lift of a heavy patient causes preventable injuries — including shoulder dislocations, falls, and fractures. Slow, supported transfers protect both the patient and the caregiver.
- Giving food, water, or oral medications before a swallowing assessment: Stroke causes dysphagia in roughly 42% of acute cases. Anything given by mouth without clearance risks life-threatening aspiration pneumonia.
- Withholding key information from EMS: Last-known-well time and current medications — especially blood thinners — directly affect treatment decisions at the hospital. Write these down before paramedics arrive if possible.
Choosing the Right Stroke Transport Option
The right transport method depends on the phase of stroke care: acute emergencies require 911/EMS, while post-hospital needs call for a different approach.
Emergency Medical Services (EMS / 911)
EMS is the only appropriate option for acute stroke. Paramedics can monitor vitals, administer oxygen, communicate with receiving facilities, and reduce door-to-treatment time.
Patients arriving by EMS are significantly more likely to receive treatment within critical time windows: 67.8% received tPA within 60 minutes compared to only 54.5% of patients arriving by private vehicle.
Non-Emergency Medical Transport (NEMT)
For stroke survivors discharged from the hospital who cannot safely ride in a private vehicle — whether due to wheelchair dependence, stretcher needs, or cognitive or physical limitations — NEMT provides specially equipped vehicles and trained staff to handle ongoing care transport safely.
AllCare Medical Transport serves Palm Coast, Flagler County, Daytona, St. Augustine, and surrounding Florida areas with 24/7 NEMT. Key service features include:
- CPR/First Aid certified, PASS-certified staff trained in wheelchair and stretcher transport
- Vehicles equipped for ambulatory assistance, wheelchair, and stretcher transport
- Coverage for rehab appointments, physician follow-ups, and facility transfers
For families coordinating post-stroke care, having a transport provider already vetted for safety and availability removes one significant variable from an already demanding process.
What to Prepare Before Transporting a Stroke Patient
Gather essential documents and information before transport:
- List of current medications (especially blood thinners or anticoagulants)
- Patient's medical history
- Insurance information
- Name of neurologist or primary care physician
- Names of sending and receiving facilities (if this is a transfer)
Confirm the destination facility has appropriate stroke capabilities for the patient's needs. For acute strokes, confirm whether the receiving hospital is a Primary Stroke Center, Comprehensive Stroke Center, or Thrombectomy-Capable Stroke Center, since only Comprehensive and Thrombectomy-Capable centers can perform advanced interventions like mechanical thrombectomy.
For non-emergency transports, logistics preparation matters just as much. Confirm in advance whether the patient requires a wheelchair, stretcher, or ambulatory assistance. Also communicate any behavioral or communication challenges — aphasia, confusion, or agitation — to the transport provider beforehand.
Conclusion
Transporting a stroke patient safely requires understanding two distinct phases: the acute emergency phase and the ongoing care phase.
During an acute stroke, call 911 immediately, note symptom onset time, and communicate clearly with EMS. For ongoing recovery, focus on safe physical handling, proper positioning, and choosing the right transport option — such as NEMT — for post-hospital needs.
The most preventable mistakes include:
- Driving to the ER instead of calling 911
- Rough or unsupported handling during transfers
- Failing to communicate symptom details to medical staff
Each of these errors is avoidable with the right preparation. For families in Florida managing post-hospital stroke transport, a licensed NEMT provider like AllCare Medical Transport can handle the logistics safely — so you can focus on recovery.
Frequently Asked Questions
What are the important time windows for acute stroke treatment (e.g., tPA and thrombectomy)?
tPA (clot-busting medication) is typically administered within 3–4.5 hours of symptom onset for eligible ischemic stroke patients, while endovascular thrombectomy (mechanical clot removal) may be an option for up to 24 hours in select cases. Faster treatment consistently leads to better outcomes.
What is the immediate priority in caring for an unresponsive or suspected stroke patient?
The immediate priority is calling 911, noting the exact time symptoms began, and keeping the patient safe and still. If unconscious and breathing, place them in the recovery position; if not breathing and trained, begin CPR.
What are the benefits of EMS transport to a stroke center for suspected acute ischemic stroke?
EMS transport allows pre-hospital assessment, advance notification of the stroke team, and direct routing to a capable stroke center. Each of these steps cuts time-to-treatment and improves recovery odds compared to arriving by private vehicle.
What is the most common complication immediately following a stroke?
Brain swelling (cerebral edema) and aspiration pneumonia (from swallowing difficulties) are among the most common immediate complications. Keeping the patient properly positioned and avoiding oral intake until a swallowing assessment is done can reduce both risks.
How long is a hospital stay after a stroke?
Hospital stays vary by stroke severity. Mild strokes may require only a few days, while more severe strokes often mean one to two weeks of acute care followed by inpatient rehabilitation.
What services are available for stroke patients after discharge?
Post-discharge services include inpatient and outpatient rehabilitation, speech/occupational/physical therapy, home health aides, and non-emergency medical transport for patients who cannot safely use personal vehicles or public transportation to attend follow-up appointments.