Introduction
Transporting a patient on a stretcher is a critical skill that directly affects patient safety and comfort across hospital discharges, non-emergency medical transport, and facility-to-facility transfers. AllCare Medical Transport handles these transports every day for seniors and medically complex patients throughout Florida, bringing 16 years of experience to every move.
While stretcher transport may seem routine, outcomes vary widely based on preparation, team coordination, patient condition, and execution. Poor technique causes injuries to both patients and transport teams.
The stakes are real: The Joint Commission reported 776 patient falls in 2024 alone, with 65% resulting in severe harm and 56% occurring among patients aged 70 and older. Equipment-related problems during transport, including accidental dislodgement of lines, tubes, and catheters, account for one-third of all safety hazards.
Getting it right requires more than physical strength — it demands the right knowledge at every stage. This guide covers when a stretcher is the right choice, what to prepare, transport steps, critical safety rules, common mistakes, and how to handle challenging scenarios.
TLDR
- Use at least 2 trained attendants, verify equipment (brakes, side rails, safety strap), and confirm team communication before moving
- Always move patients feet-first—except when entering an elevator or emergency room where head-first entry applies
- Proper body mechanics (power lift, straight back, weight close to body) protect both patients and transport teams from injury
- Secure all IV lines, catheters, and monitoring equipment before movement — and never leave a patient unattended on a stretcher
- For medically complex patients, use PASS-certified transport professionals
Preparation: When a Stretcher Is Needed and What to Check First
Not every patient requires a stretcher. Stretcher transport is most appropriate for patients who cannot sit upright safely, require a supine position during transport (post-surgical, spinal injury, cardiac monitoring), or are non-ambulatory due to weakness, injury, or medical status.
CMS defines a patient as "bed-confined" when they meet all three criteria:
- Unable to get up from bed without assistance
- Unable to ambulate
- Unable to sit in a chair or wheelchair
Additional indications include contractures, non-healed fractures, severe pain on movement, deep vein thrombosis requiring limb elevation, or orthopedic devices needing special handling. Wheelchair transport, by contrast, is appropriate when the patient can bear weight and maintain an upright sitting position.
Equipment and Stretcher Checks
Before any transport, verify the stretcher functions correctly:
- Test wheel locks (brakes) to ensure they engage fully
- Confirm side rails raise and lower properly without catching or binding
- Check the safety strap is intact and can be secured without pressing on the patient's abdomen
- Ensure the head section elevates as needed for patient comfort
- Verify weight capacity—standard stretchers support up to 700 lbs, while bariatric models handle 850-1,600 lbs
Standard transport stretchers from manufacturers like Stryker Power-PRO 2 and Hillrom max out at 700 lbs Safe Working Load (SWL), whereas specialized bariatric cots support 850–1,600 lbs depending on the model. Always confirm the specific model's rating — numbers on the side of the cot can differ from catalog specs.
Patient Assessment and Pre-Transport Checklist
Complete the pre-transport checklist before moving the patient:
- Confirm patient identity using two identifiers
- Assess airway, breathing, and circulation (ABCs)
- Secure all IV lines, catheters, and drainage bags below the patient's level
- Verify monitoring leads are connected and functioning
- Communicate the plan clearly to the patient so they know what to expect and how they can assist (crossing arms over chest, keeping hands inside rails)
A 2014 NEJM study on standardized handoff protocols found a 23% reduction in medical errors and a 30% drop in preventable adverse events — evidence that the pre-transport conversation is as important as the physical transfer itself.

How to Transport a Patient on a Stretcher: Step-by-Step
Step 1: Prepare the Patient and Workspace
Position the patient toward the edge of the surface they're being moved from. Lower guard rails and adjust the surface to the appropriate working height—level with the stretcher or slightly higher to assist the slide. Place a friction-reducing device (slider board with sheet) under the patient if transferring from a bed.
Laboratory studies show that air-assisted devices reduce hand pull force by approximately 69% compared to traditional draw sheets (40 N vs 128 N), cutting spinal compression forces on the transport team.
Instruct the patient to cross their arms over their chest and tuck their chin. Communicate each action before performing it—this reduces anxiety and encourages cooperation, particularly for geriatric or cognitively impaired patients.
Step 2: Position the Team and Transfer the Patient to the Stretcher
Once the patient is ready, assign roles before the move begins. Clear role assignments prevent hesitation mid-transfer:
- One attendant at the head stabilizes the head and shoulders, and calls the count
- One or two attendants at mid-torso grip the draw sheet from the stretcher side
- One attendant at the foot supports the lower extremities
On the team leader's count, slide (not lift) the patient across to the stretcher center using coordinated weight shifts. The push-pull method reduces spinal load on the team.
Use proper body mechanics throughout:
- Keep back upright and straight
- Bend at the knees (power lift position)
- Keep the load close to the body
- Avoid twisting the spine during the transfer
The NIOSH lifting equation limits safe manual lifting to 35 lbs under ideal conditions. When manually repositioning patients, spine compression and hand forces frequently exceed recommended limits, making friction-reducing devices and proper technique essential.

Step 3: Secure the Patient and Adjust the Stretcher
Once the patient is centered on the stretcher:
- Raise both side rails immediately
- Apply the safety strap across the thighs (not the abdomen)—the strap should allow two fingers to slide underneath
- Confirm all lines and tubes are untangled and properly positioned
- Raise the stretcher to rolling height (approximately 32-36 inches)
- Confirm brakes are released only when the team is ready to move
Verbally confirm with the patient that they are comfortable. Pad bony prominences (hips, heels, shoulders) to prevent pressure injuries during longer transports—this is especially critical for geriatric or hospice patients.
Step 4: Transport and Arrive at Destination
Move the stretcher feet-first: one attendant leads at the foot end while another stays at the patient's head, guiding the move and monitoring the patient throughout. Avoid rapid movements and wide corner swings—sudden acceleration can cause dizziness, disorientation, or nausea, particularly in patients who have received medications.
On arrival:
- Lock the stretcher brakes before transferring the patient
- Lower the guard rails only when ready to perform the transfer
- Never leave the patient unattended on the stretcher at any point during or after transport
Key Safety Rules Every Stretcher Transport Must Follow
These rules exist because even experienced transport teams can cause patient falls, line disconnections, or staff injuries when protocols slip. Following them consistently is what makes a transport safe.
Team Size and Weight Limits
A minimum of 2 trained attendants is required for standard transport. The Association of Surgical Technologists (AST) mandates that for semi-conscious, unconscious, or nonmobile patients, a minimum of four personnel is required.
Team size requirements:
- Standard transport: 2 trained attendants minimum
- Patients over 250 lbs: 4 attendants recommended
- Stair navigation: 4 personnel total (2 operators plus 2 helpers)
- Bariatric patients: Position strongest attendants at head and foot

Standard stretchers are typically rated up to 700 lbs, while bariatric models support 850–900 lbs. Verify current manufacturer specifications before loading any patient.
Patient Is Never Left Unattended
Liability for the patient's health and wellbeing rests with the transport team for the full duration of the transport. One attendant must remain with the patient at all times — including elevator waits and hallway delays.
Coordinated Verbal Commands
The team leader must give preparatory counts ("1, 2, 3") before any lift, shift, or move. All team members must understand whether the action starts on "3" or after "3." Breakdowns in communication are a leading cause of patient drops and team injuries.
Certification and Training Matter
When booking a non-emergency transport, credentials tell you whether a provider actually follows these protocols — or just says they do. AllCare Medical Transport, for example, holds PASS certification (wheelchair and stretcher), CPR/First Aid credentials, and requires all personnel to pass DOT physicals, drug tests, and national and local background checks.
Before booking any provider, ask specifically about PASS certification, CPR/First Aid currency, background check procedures, and current liability insurance coverage.
Common Mistakes When Transporting Patients on a Stretcher
Skipping the Pre-Transport Checklist
Rushing past equipment checks—unlocked brakes, unsecured side rails, unverified line placement—accounts for a large share of preventable transport incidents. When IV lines are accidentally disconnected or a stretcher rolls because brakes aren't locked, patient harm and treatment delays result.
Equipment-related problems, including accidental dislodgement of lines, tubes, and catheters, are prominent causes of intrahospital transport adverse events.
Using Incorrect Body Mechanics or Insufficient Team Members
A single attendant attempting to lift or reposition a patient, or lifting with a bent and twisted back, leads to back injuries and patient instability. In 2023-2024, healthcare support occupations experienced an annualized Days Away from Work incidence rate of 32.4 per 10,000 FTE workers for musculoskeletal disorders—the leading cause of missed workdays among healthcare workers.
Safe horizontal transfers follow a few non-negotiable rules:
- Minimum 2 attendants required for every patient transfer
- Position the bed at the mid-thigh height of the shortest lifter
- Begin in a squat with a neutral spine—never bend and twist simultaneously
- Apply the power lift principle throughout the move
Ignoring Patient Condition and Positioning Needs
Some patients cannot lie flat due to respiratory compromise or certain post-surgical cases. Failing to elevate the head of the stretcher to the appropriate angle, or placing a safety strap over the abdomen, can directly worsen the patient's medical status.
The strap should allow two fingers to slide underneath it and should sit across the thighs, not the abdomen. For patients requiring elevated positioning, adjust the head section before transport begins and reconfirm comfort after securing the patient.
Special Scenarios: Navigating Elevators, Stairs, and High-Weight Patients
Elevator Protocol
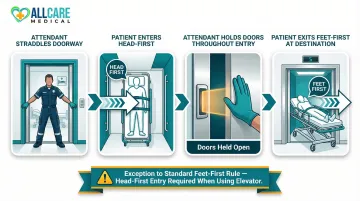
When entering an elevator, have one attendant straddle the doorway to prevent the doors from closing on the patient or stretcher. The Association of Surgical Technologists explicitly mandates that stretchers enter elevators head-first as an exception to the standard feet-first transport rule.
Elevator entry procedure:
- Patient enters head-first into the elevator
- One attendant holds doors open throughout entry
- The attendant at the head always monitors the patient's airway and can respond immediately to respiratory distress
- Patient exits feet-first once doors open at the destination floor
Stair Navigation
Wheeled stretchers are too heavy for safe stair use with a patient on board. A stair chair or backboard is the preferred alternative. Manufacturer guidelines (Stryker) dictate that "Changing Levels" (such as stairs) with an occupied cot requires two operators and two helpers (four personnel total).
If a stretcher must be used on inclines:
- Keep it as level as possible
- Position the shorter attendant on the lower end
- Ensure the patient is tightly secured to prevent sliding
- Always carry backboards or stretchers foot-end first so the patient's head remains elevated above the feet
When a stair chair is required, assign a spotter who keeps one hand on the back of the carrier and calls out turns and landings throughout the descent or ascent.
Bariatric and High-Weight Patients
CDC data from August 2021 to August 2023 indicates U.S. adult obesity prevalence is 40.3%, with severe obesity at 9.4%. This means NEMT providers should use bariatric-rated stretchers and expanded teams.
For patients over 250 lbs:
- Use four attendants (strongest at the head and foot)
- Verify the stretcher's weight-rated capacity before transport
- Consider mechanical lift assistance for ambulance loading
- Deploy bariatric stretchers with wider platforms (up to 37.4 inches with extenders) and wider wheelbases for stability
AllCare Medical Transport is PASS-certified for both wheelchair and stretcher transport and operates 24/7 across Florida — including bariatric transport scenarios that require specialized equipment and additional personnel.
Frequently Asked Questions
How do you transport a patient on a stretcher?
Secure the patient with the safety strap across the thighs and raise both side rails. At least two attendants then move the stretcher feet-first—one at the head monitoring the patient, one guiding at the foot—with all lines and equipment secured before movement begins.
Which technique is appropriate for moving a patient to a stretcher?
The draw sheet or slide board method is most commonly used for bed-to-stretcher transfers, using a friction-reducing board under a sheet. The team positions on either side and slides the patient across on a coordinated count rather than lifting the full body weight, reducing spinal compression by up to 69%.
When transporting a surgical patient on a stretcher, how should the stretcher be positioned on an elevator?
The patient enters the elevator head-first (one of two exceptions to the feet-first transport rule). An attendant holds the elevator doors open, the stretcher is pushed in with the patient's head leading, and the patient exits feet-first once the doors open at the destination floor.
Why do stretchers require padding when transporting a patient?
Padding protects bony prominences (hips, heels, shoulders, back of head) from pressure injuries that can develop even during short transports, particularly in geriatric, frail, or immobile patients. It also improves patient comfort and reduces agitation during longer non-emergency transports.
How many people are needed to safely transport a patient on a stretcher?
A minimum of 2 trained attendants are required for standard stretcher transport. This increases to 4 for patients over 250 lbs, those requiring stair navigation, or critically ill patients with complex equipment attached.
What is the difference between urgent and non-urgent stretcher transport?
Urgent moves prioritize rapid relocation when life-threatening conditions exist (altered consciousness, shock, scene hazard) and may compress some immobilization steps. Non-urgent moves (such as hospital discharges or medical appointments) allow full preparation, proper positioning, and unhurried execution for maximum patient safety and comfort.
Need professional stretcher transport in Florida? AllCare Medical Transport provides PASS certified, CPR/First Aid trained personnel for safe, comfortable stretcher transport 24/7. Contact us at (386) 864-7145 or email info@allcaremedicaltransport.com for a free consultation.