Introduction
Each day across the U.S., thousands of family caregivers and home health aides face one of the most physically demanding caregiving tasks: helping a patient with limited mobility transfer from their bed to a wheelchair. The risk is real. In 2020 alone, nursing assistants experienced 96,480 nonfatal injury cases involving days away from work, with overexertion during lifting accounting for a significant portion of these injuries.
Improper transfer technique is a leading cause of both caregiver back injuries and patient falls. Nearly 60% of manual wheelchair users experience falls, many occurring during transfers. This guide covers the correct transfer process step by step: patient assessment, choosing the right method, proper body mechanics, and the common mistakes that cause injuries.
TL;DR
- Assess the patient's weight-bearing ability before every transfer ; what worked yesterday may not be safe today
- Lock the wheelchair, position it on the patient's stronger side, and clear all obstacles before starting
- Use the pivot turn for patients who can bear weight on at least one leg; always use a gait belt for a secure grip
- Non-weight-bearing patients require a mechanical lift or transfer board; a standing pivot is not safe for them
- When professional help is needed, choose a PASS-certified NEMT provider — their staff are trained specifically in safe wheelchair and stretcher transfers
Why Transfer Safety Matters — and How to Prepare
The Real Cost of Unsafe Transfers
Manual patient handling causes severe injuries for both caregivers and patients. Research shows that 12% of home health aides reported at least one work-related injury in a 12-month period, with back injuries (44%) and strains (43%) being the most common. For patients, the stakes are equally high: observational data reveals that 70.7% of wheelchair falls are caused by incorrect transfers or body weight shifts.
The myth of "proper body mechanics" persists, but bending your knees and keeping your back straight cannot eliminate injury risk when lifting another adult.
The National Institute for Occupational Safety and Health (NIOSH) recommends caregivers manually lift no more than 35 pounds of a patient's weight under ideal conditions. Exceeding that threshold requires mechanical assistive devices — not just better technique.
Pre-Transfer Assessment Checklist
Before attempting any transfer, evaluate:
Patient's Physical Ability:
- Can they bear weight on at least one leg?
- Do they have adequate sitting balance and upper-body strength?
- Can they follow multi-step verbal instructions?
- Are there medical contraindications (recent surgery, fragile bones, active dizziness)?
Environment and Equipment:
- Wheelchair brakes locked and tested
- Footrests swung away or removed
- Armrests removed, folded, or lowered
- Loose rugs and obstacles cleared from path
- Bed lowered to appropriate height (patient's feet flat on floor when seated)
- Non-skid footwear on patient
- Gait belt or transfer board within reach
Caregiver Capability:
- Are you physically able to support the patient's weight?
- Is a second person available if needed?
- Do you understand the technique and feel confident?
Step-by-Step: How to Move a Patient from Bed to Wheelchair
The following steps describe the standard pivot transfer — the most common technique for patients who can bear weight on at least one leg.
If the patient cannot bear any weight, skip to the section on mechanical lifts below. Attempting a pivot transfer on a non-weight-bearing patient is unsafe and risks injury to both caregiver and patient.
Step 1: Position the Wheelchair and Explain the Process
Place the wheelchair on the same side as the patient's stronger leg, angled at a 45-degree angle to the bed. Lock both wheels and verify they're secure by attempting to push the chair. Remove or fold back the footrests and armrests to create clear entry space.
Explain each step to the patient before you begin: "I'm going to help you sit up, then move to the edge of the bed, then stand and pivot into your wheelchair." Confirm they understand and are ready. This reduces anxiety and improves cooperation throughout the transfer.
Step 2: Bring the Patient to a Seated Position
Roll the patient onto their side facing the wheelchair. Place one arm under their shoulders and one behind their knees, then swing their legs off the edge of the bed in one smooth, controlled motion while helping them sit upright.
Critical pause: Let the patient remain seated at the edge for at least 30 seconds (ideally 3 minutes if time permits) to check for dizziness. This "dangle protocol" prevents orthostatic hypotension (sudden blood pressure drop) that causes fainting during transfers.
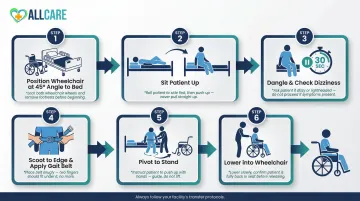
Step 3: Move the Patient to the Edge of the Bed
Help the patient scoot forward until their feet are flat on the floor and their knees are bent at approximately 90 degrees. Lower the bed if necessary to achieve full foot contact with the ground.
With the patient positioned at the edge, this is the right moment to apply a gait belt if you're using one. Wrap it snugly around the natural waist with enough room to barely fit two fingers underneath. Never place the belt over surgical sites, colostomies, or chest tubes.
Step 4: Help the Patient Stand Using the Pivot Technique
Stand directly in front of the patient with your feet shoulder-width apart and knees slightly bent. Place the patient's outside leg (farthest from the wheelchair) between your knees for support and stability.
Then execute the lift in sequence:
- Reach around the patient's torso and grasp the gait belt firmly with an underhand grip (never let the patient grab your neck — this risks falls and injury for both of you)
- Count to three aloud, then rise together using your leg muscles while keeping your back straight
- Cue the patient to push off the bed with both hands and lean forward ("nose over toes") as they stand
Step 5: Pivot Toward the Wheelchair
With the patient standing and bearing weight on their stronger leg, pivot together in small steps toward the wheelchair. Move your feet rather than twisting at the waist. Continue pivoting until the back of the patient's legs are touching the wheelchair seat.
Critical safety note: If the patient begins to fall at any point, do not attempt to hold them upright. Instead, lower them gently to the nearest flat surface (bed, floor, or chair) by bending your knees and controlling the descent.
Step 6: Lower the Patient Into the Wheelchair and Adjust Position
Ask the patient to reach for the wheelchair armrest with their inside hand. Bend your knees to lower them into the seat, controlling the descent rather than dropping them.
Once seated, ensure:
- Hips are pushed all the way back in the seat
- Feet are positioned on the footrests
- Patient is centered and comfortable
- Lap belt is secured if needed
Do not release your hold until you confirm the patient is stable and properly positioned.
Choosing the Right Transfer Method for Your Patient
Not every patient can safely perform a pivot transfer. The correct technique depends on the patient's weight-bearing ability, upper body strength, cognitive status, and overall mobility. Using the wrong method is one of the most common causes of transfer injuries.
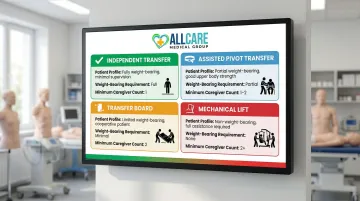
The Four Transfer Types
| Transfer Type | Patient Can Do | Equipment | Caregivers |
|---|---|---|---|
| Independent | Full weight-bearing, maintains balance, no assistance needed | Locked wheelchair | Standby only |
| Assisted Pivot | Bear weight on one leg, follow instructions, maintain sitting balance | Gait belt | 1 (if lifting <35 lbs) |
| Transfer Board | Upper body strength and sitting balance; no leg weight-bearing (e.g., paraplegia, bilateral amputation) | Sliding board, gait belt | 1–2 |
| Mechanical Lift | Fully dependent, non-weight-bearing, severe spasticity, or exceeds manual lift threshold | Hoyer lift or sit-to-stand lift | 2 minimum |
When to Use a Gait Belt
Use a gait belt for most assisted pivot transfers — it provides a firm grip on the patient's torso without straining their arms or shoulders.
Proper use:
- Position the belt around the patient's natural waist (not hips or chest)
- Tighten until you can fit two fingers underneath
- Grasp with an underhand grip
- Use the belt to steady and guide — not to lift the patient's full weight
Not every patient can tolerate a gait belt. Skip it entirely for patients with:
Contraindications:
- Recent abdominal, chest, or back surgery
- Colostomies, ileostomies, or feeding tubes
- Chest tubes or severe respiratory conditions
- Abdominal aortic aneurysms
- Severe cardiac conditions
When a gait belt isn't safe and manual support isn't enough, a mechanical lift becomes necessary.
When a Mechanical Lift Is Required
NIOSH guidelines are clear: if a manual transfer requires the caregiver to lift more than 35 pounds of the patient's weight, a mechanical lift must be used. Attempting manual transfers beyond this threshold causes the majority of caregiver back injuries.
Mechanical lifts are also required when:
- The patient is fully non-weight-bearing
- The patient is combative, unpredictable, or cannot follow instructions
- The patient has severe spasticity or contractures
- The caregiver cannot safely manage the patient's weight
Important: Always use two caregivers when operating a mechanical lift, and ensure the sling type matches both the patient's needs and the lift's hanger bar specifications. Mismatched equipment has led to serious injuries and even fatalities.
Reassess Regularly
A patient's transfer needs are not static. Reassess the appropriate method after any acute change:
- Recent surgery or hospitalization
- Falls or near-falls during previous transfers
- Changes in mental status or medication
- Illness or new diagnosis
- Noticeable decline in strength or balance
If any of these changes apply, a physical therapist can formally reassess the patient's weight-bearing status and prescribe the correct transfer method before the next move.
Common Mistakes Caregivers Make During Patient Transfers
Understanding what not to do is as important as mastering proper technique. These errors account for the majority of transfer-related injuries.
Dangerous Technique Errors
- Twisting at the waist causes rotational spinal stress — the leading source of caregiver back injuries. Move your feet in small steps and keep your torso aligned with your hips.
- Bending from the waist shifts the load to your lumbar spine. Keep your back straight and bend at the knees to engage your stronger leg muscles.
- Letting the patient grab your neck pulls you off-balance and strains both parties. Instruct patients to push off the bed or grip the wheelchair armrest instead.
- Rushing the standing phase — skipping the pause after sitting up or moving before the patient is stable — frequently causes falls from orthostatic hypotension.
Preparation Mistakes That Increase Risk
- Not locking the wheelchair: Video analysis found improper brake positioning contributed to 67.2% of wheelchair falls during transfers. Lock both wheels and test them before starting.
- Positioning the chair on the weaker side forces the patient to pivot toward their weak leg — always place it on the stronger side.
- Skipping verbal instructions leaves patients unprepared; clear, step-by-step cues throughout the transfer reduce falls.
- Moving from lying to standing without a seated pause triggers sudden blood pressure changes that can cause fainting.

The "It Worked Yesterday" Fallacy
Many caregivers assume a technique that worked before will always work. With elderly patients, that's a risky assumption — strength, balance, and blood pressure can shift daily based on hydration, medication timing, sleep quality, or a minor illness.
Reassess before every transfer, watch for signs of weakness or dizziness, and be ready to adjust your approach or call for help.
When to Seek Professional Help for Patient Transport
Some situations require more than good technique — they require professional assistance. Recognizing when a transfer is beyond your capability protects both you and the patient from serious injury.
Signs You Should Not Transfer Alone
Do not attempt a bed-to-wheelchair transfer if:
- The patient is fully non-weight-bearing and no mechanical lift is available
- The patient is significantly heavier than you can safely manage (remember the 35-lb lifting threshold)
- The patient has a documented history of falls during transfers
- You have an existing back, shoulder, or other injury that limits your lifting ability
- The patient is combative, confused, or unable to follow instructions
- You feel uncertain or unsafe about any aspect of the transfer
In these situations, getting a second person or professional assistance is the responsible choice — not a failure.
When to Use Professional Non-Emergency Medical Transport
For patients who require regular transport to medical appointments, dialysis sessions, rehabilitation therapy, or other healthcare visits, professional non-emergency medical transport (NEMT) removes the physical burden and safety risk from family caregivers.
PASS-certified NEMT providers like AllCare Medical Transport employ specialists who hold wheelchair and stretcher certification, CPR/First Aid credentials, and pass DOT physicals and background checks. They operate wheelchair-accessible vehicles with securement systems that meet ADA safety standards.
This service is particularly valuable for:
- Hospital discharge patients transitioning home or to rehabilitation facilities
- Dialysis patients requiring multiple weekly transports
- Seniors in Florida with regular medical appointments
- Patients with progressive conditions whose transfer needs change frequently
- Caregivers who lack the physical strength for safe transfers
AllCare Medical Transport serves Flagler County, Palm Coast, St. Augustine, Daytona, and surrounding Florida areas with 24/7 wheelchair and stretcher transport. Their fully licensed, insured team handles the physical demands of each trip — so family members can focus on support rather than safety logistics.
Build a Sustainable Care Plan
Attempting unsafe transfers out of necessity or convenience is one of the most preventable causes of patient injury. Caregiver injuries don't just affect you — they disrupt the patient's entire care routine.
Build a care plan that includes professional transport when appropriate, rather than relying solely on untrained family assistance. When the right resources are in place, patients get to their appointments consistently — and caregivers stay healthy enough to keep showing up.
Frequently Asked Questions
What is the proper way to transfer a patient from a bed to a wheelchair?
Assess the patient's weight-bearing ability, then position the locked wheelchair on their stronger side. Bring them to sitting at the edge of the bed and pause to check for dizziness. Use a gait belt for grip and a pivot turn technique to help them stand, pivot toward the chair, and lower into the seat.
What to avoid when moving a patient from bed to wheelchair?
Never twist at your waist — pivot your feet instead. Do not let the patient grab your neck. Always lock the wheelchair brakes before beginning. Never attempt a standing pivot on a patient who cannot bear weight; use a mechanical lift instead.
What is the correct wheelchair positioning for a transfer from bed to wheelchair?
Place the wheelchair on the patient's stronger side at a 45-degree angle to the bed. Lock both wheels, remove or fold the armrests, and swing the footrests out of the way to create clear entry space for the patient's body.
What are the 4 types of patient transfer?
The four main types are:
- Independent transfer — patient moves unassisted
- Assisted pivot transfer — caregiver supports a partially weight-bearing patient
- Transfer board/lateral transfer — for patients who cannot stand but can shift weight
- Mechanical lift transfer — for fully dependent patients
The right method depends on the patient's weight-bearing capacity.
How to transport a person in a wheelchair?
Ensure the patient is fully seated with their hips back, feet on the footrests, and a lap belt secured if available. Use ramps instead of stairs, and confirm the wheelchair is locked whenever the vehicle is stationary. For longer or medical trips, a licensed NEMT provider with wheelchair-accessible vehicles and trained staff offers the safest option.
Need 24/7 wheelchair transport in Florida? AllCare Medical Transport provides PASS-certified wheelchair and stretcher transport throughout Flagler County, Palm Coast, St. Augustine, Daytona, and surrounding areas. Call (386) 864-7145 or visit allcaremedicaltransport.com for a free quote.